This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I did an informal poll on Twitter and less than half of respondents ranked HPM in the top 10. Additionally, we are still quite a young specialty, with the birth of HPM as an official specialty being announced in 2005 , and getting started in 2008. by Christian Sinclair ( @ctsinclair ) We have entered a new age! Spread the word!
This continued in the setting of medical specialist training where even more information was memorised and regurgitated during exams. They would all come back together to present their information to each other. Garnering opinions and information from team members rather than all working completely independently. Cashman et al.
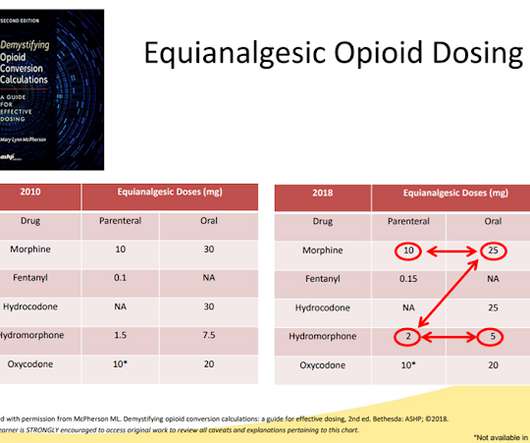
by Drew Rosielle ( @drosielle ) I am proposing we do away with equianalgesic table (EAT) as a tool to inform clinical decisions about opioid rotations/conversions. He founded Pallimed in 2005. Fundamentally, EATs create too many problems, and there are simpler and safer ways to teach clinicians how to convert between different opioids.
The cohort study analyzed site-of-death data from 2005 through 2017, including more than 7.5 The cohort study analyzed site-of-death data from 2005 through 2017, including more than 7.5 Recent research has found that varying state laws around palliative care can impact cancer patients’ place of death.
That was in 2005. I’m curious as to how that learning experience may have informed your approach to educating others about hospice. The mobile practice is focused on caring for patients who have been discharged alive from hospice until they once again are deemed eligible. G’s H.O.S.P.I.C.E She’s also launched a podcast, “Dr.
6 Anecdotal information shows that patients with incurable cancer often do not perceive themselves as “palliative”, a connotation they more commonly associate with impending death. Instead, these patients often prefer the word “chronic.” Although palliative approaches (e.g., Instead, these patients often prefer the word “chronic.”
But we can’t lose sight of the system level, the x individual outside of the individual, the system level factors that inform our day to day workplace experience. That was like 2005. Alex 00:15 We are delighted to welcome Jane deLima Thomas, who was a co-fellow with me back in the day in palliative care. Thanks for having me.
Amanda Sternklar ( 00:54 ): Marissa has been working in public relations and marketing for over 15 years with a focus on in-home care marketing since 2005 when working for one of Washington state’s top public relations firms. But we’re not just talking about any information. She won the Wind Beneath Our Wings Award.
In 2005, Gary Franklin, MD, MPH, Director of the Labor and Industry Program, who would later become PROP’s Vice President of State Regulatory Affairs, published an article alleging that “that tolerance or opioid-induced abnormal pain sensitivity may be occurring in some workers who use opioids for chronic pain (9).”
The more interested they are the more they are likely to retain information that could be useful to their future patients. Describe the context and rationale for your plan of integrating digital and collaborative learning into your practice Education is what remains after one has forgotten everything he learned in school.
I can't help them make informed care decisions otherwise, and honestly I'm less interested in outcomes research focused on if I should be talking with my patients about the future than how I should be talking with them about the future. He founded Pallimed in 2005. For more Pallimed posts by Dr. Rosielle click here.
Dealing with conflict in caring for the seriously ill: “it was just out of the question” JAMA 2005. So, from my standpoint, what I always tell people is to get as much information as possible, so talk to other family members, make sure everybody is on the same kind of pathway. Journal of Patient Experience. December 2020.
by Chad Kollas, MD ( @ChadDKollas ) Introduction A recent study by the Centers for Disease Control (CDC) has captured the attention of the palliative care and chronic pain communities (1). The Backlash to the PROP Petition Begins This unity within the supporters of the petitioning group was short-lived.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content